Dcfs Medical Form - This form is for legal custodians/guardians of minors who authorize ordinary and routine medical and/or dental care by dcfs. Feel free to copy these forms as needed. Health care provider (md, do, apn, pa, school health professional, health official) verifying above immunization history must sign below. Forms are available for view in either or both of the following formats: This form will aid the department in determining the physical wellness and capabilities of adults in foster or adoptive homes who are or may be. If you have a question about a form in particular,. The day and month is required if. This page includes all dcfs forms available online. Note the mo/da/yr for every dose administered. To be completed by health care provider.
Forms are available for view in either or both of the following formats: To be completed by health care provider. Feel free to copy these forms as needed. If you have a question about a form in particular,. The day and month is required if. This form will aid the department in determining the physical wellness and capabilities of adults in foster or adoptive homes who are or may be. This form is for legal custodians/guardians of minors who authorize ordinary and routine medical and/or dental care by dcfs. Health care provider (md, do, apn, pa, school health professional, health official) verifying above immunization history must sign below. Note the mo/da/yr for every dose administered. This page includes all dcfs forms available online.
This form will aid the department in determining the physical wellness and capabilities of adults in foster or adoptive homes who are or may be. If you have a question about a form in particular,. Note the mo/da/yr for every dose administered. This page includes all dcfs forms available online. The day and month is required if. Feel free to copy these forms as needed. Forms are available for view in either or both of the following formats: This form is for legal custodians/guardians of minors who authorize ordinary and routine medical and/or dental care by dcfs. Health care provider (md, do, apn, pa, school health professional, health official) verifying above immunization history must sign below. To be completed by health care provider.
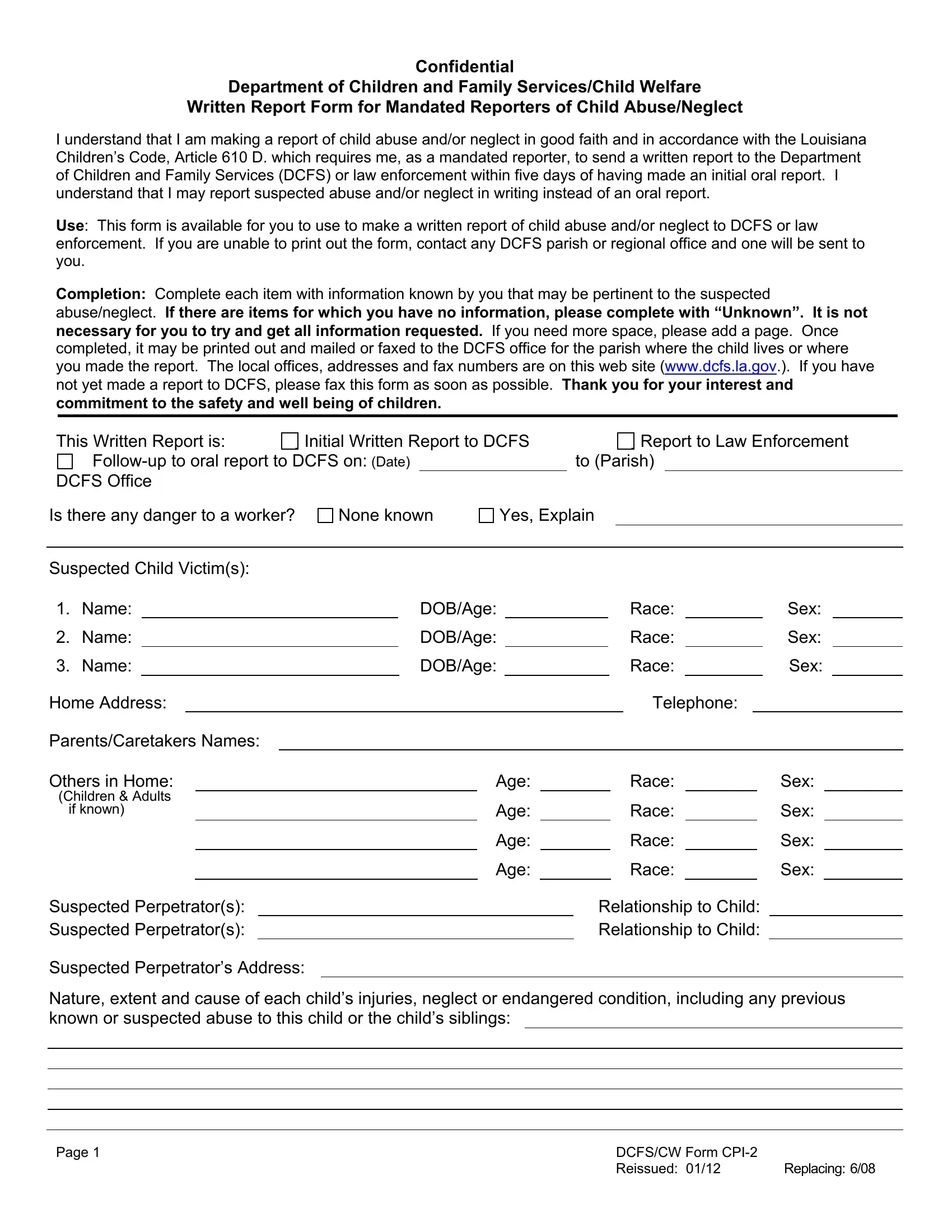
Dcfs Cw Form Cpi 2 ≡ Fill Out Printable PDF Forms Online
This form is for legal custodians/guardians of minors who authorize ordinary and routine medical and/or dental care by dcfs. This form will aid the department in determining the physical wellness and capabilities of adults in foster or adoptive homes who are or may be. Note the mo/da/yr for every dose administered. This page includes all dcfs forms available online. Feel.

food stamp application print 20152024 Doc Template pdfFiller
Note the mo/da/yr for every dose administered. This form is for legal custodians/guardians of minors who authorize ordinary and routine medical and/or dental care by dcfs. To be completed by health care provider. Forms are available for view in either or both of the following formats: The day and month is required if.
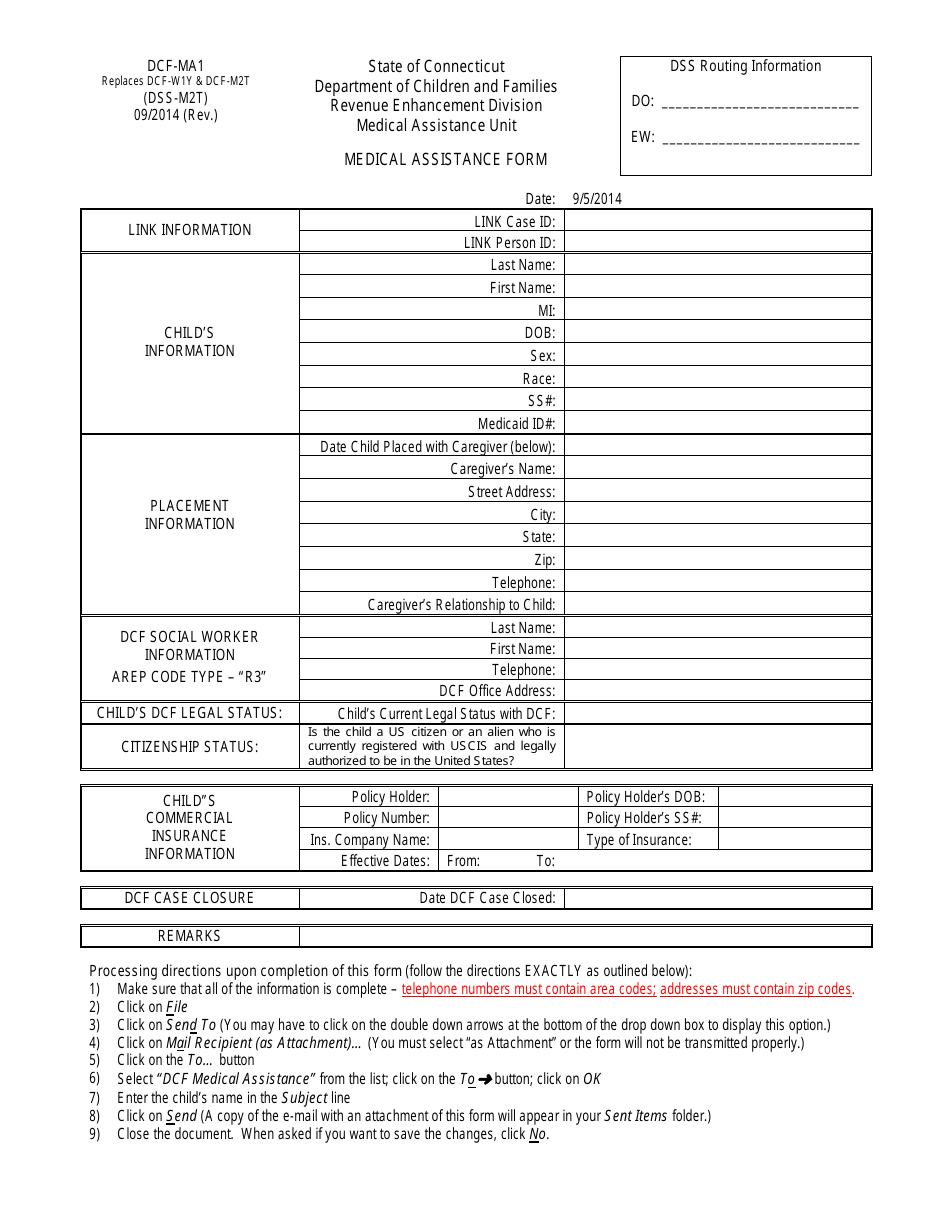
Form DCFMA1 Fill Out, Sign Online and Download Printable PDF
This page includes all dcfs forms available online. To be completed by health care provider. Feel free to copy these forms as needed. This form will aid the department in determining the physical wellness and capabilities of adults in foster or adoptive homes who are or may be. Health care provider (md, do, apn, pa, school health professional, health official).
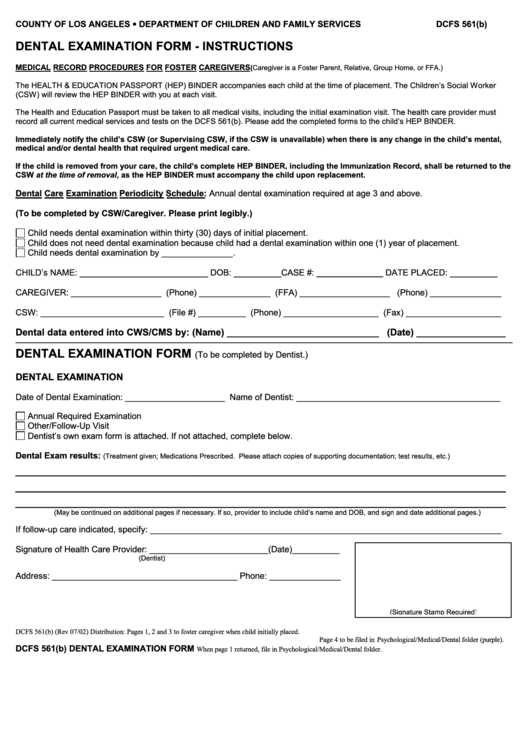
Form Dcfs 561(B) Dental Examination Los Angeles Dcfs printable pdf
If you have a question about a form in particular,. This form is for legal custodians/guardians of minors who authorize ordinary and routine medical and/or dental care by dcfs. Health care provider (md, do, apn, pa, school health professional, health official) verifying above immunization history must sign below. The day and month is required if. Forms are available for view.
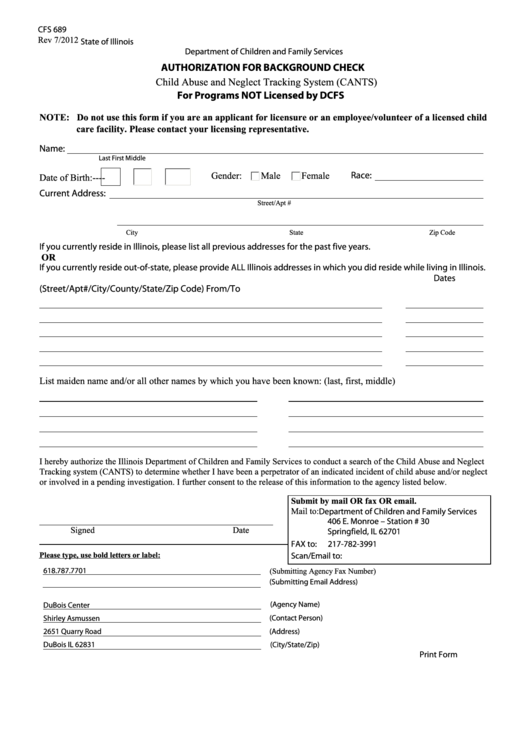
Fillable Dcfs Form Dubois Center printable pdf download
Note the mo/da/yr for every dose administered. If you have a question about a form in particular,. This form is for legal custodians/guardians of minors who authorize ordinary and routine medical and/or dental care by dcfs. Forms are available for view in either or both of the following formats: The day and month is required if.

DCFS Medical Lens IRR PDF Substance Abuse Mental Disorder
Note the mo/da/yr for every dose administered. To be completed by health care provider. The day and month is required if. Forms are available for view in either or both of the following formats: This form is for legal custodians/guardians of minors who authorize ordinary and routine medical and/or dental care by dcfs.

Fillable Online Dcfs Employee Physical Form. Dcfs Employee Physical
Feel free to copy these forms as needed. This page includes all dcfs forms available online. Health care provider (md, do, apn, pa, school health professional, health official) verifying above immunization history must sign below. To be completed by health care provider. Note the mo/da/yr for every dose administered.

Dcfs Medical Consent Form 2024 Printable Consent Form 2024
This page includes all dcfs forms available online. Feel free to copy these forms as needed. This form will aid the department in determining the physical wellness and capabilities of adults in foster or adoptive homes who are or may be. The day and month is required if. If you have a question about a form in particular,.

Dcfs Medical Consent Form Printable Consent Form 2022
This form will aid the department in determining the physical wellness and capabilities of adults in foster or adoptive homes who are or may be. Health care provider (md, do, apn, pa, school health professional, health official) verifying above immunization history must sign below. Note the mo/da/yr for every dose administered. If you have a question about a form in.
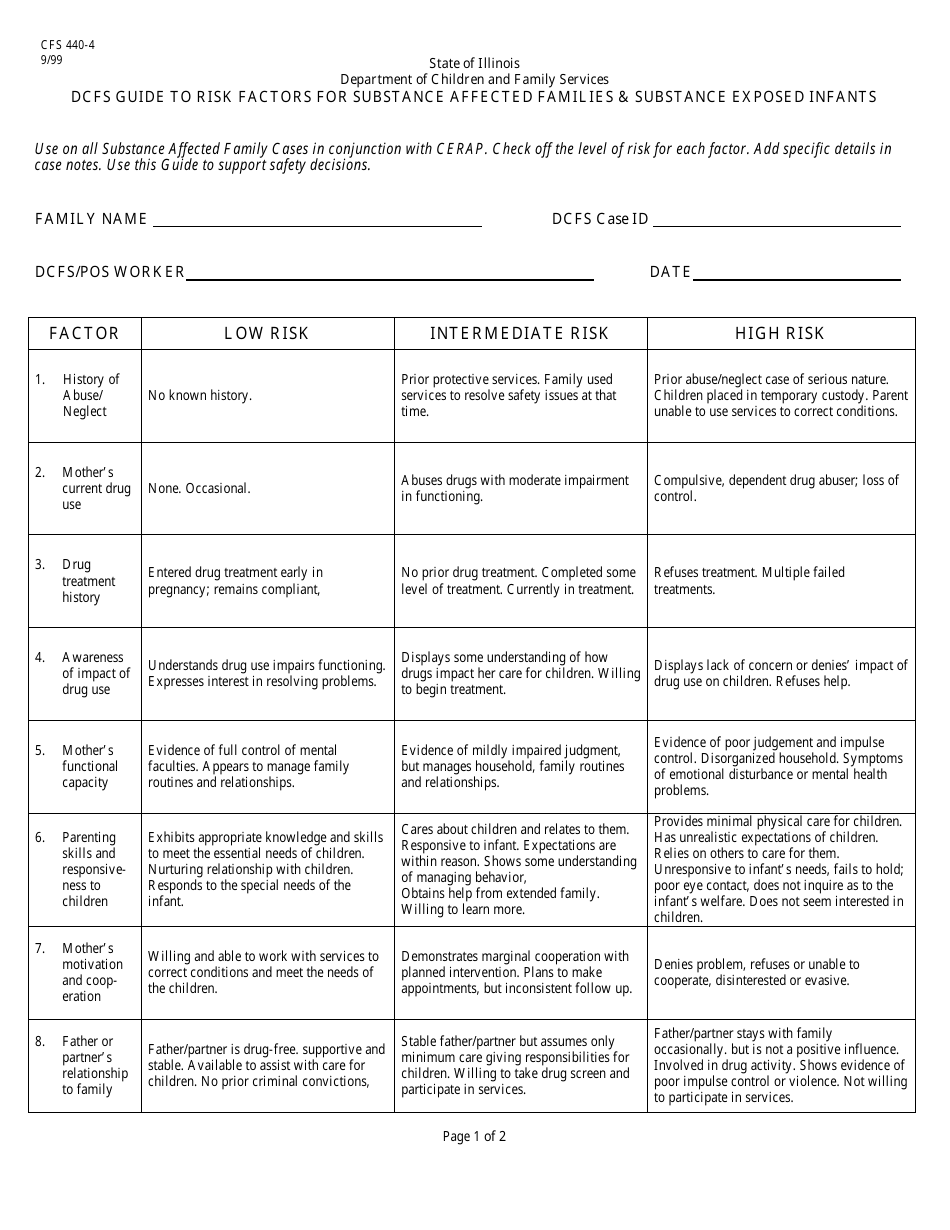
Form CFS4404 Fill Out, Sign Online and Download Fillable PDF
The day and month is required if. This form is for legal custodians/guardians of minors who authorize ordinary and routine medical and/or dental care by dcfs. Note the mo/da/yr for every dose administered. To be completed by health care provider. This page includes all dcfs forms available online.
The Day And Month Is Required If.
Health care provider (md, do, apn, pa, school health professional, health official) verifying above immunization history must sign below. This form is for legal custodians/guardians of minors who authorize ordinary and routine medical and/or dental care by dcfs. If you have a question about a form in particular,. This page includes all dcfs forms available online.
To Be Completed By Health Care Provider.
Forms are available for view in either or both of the following formats: This form will aid the department in determining the physical wellness and capabilities of adults in foster or adoptive homes who are or may be. Note the mo/da/yr for every dose administered. Feel free to copy these forms as needed.